



“The disease spreads through very close personal contact, blood and feces,” explained Harvard Humanitarian Initiative Director Michael VanRooyen (left).
File photo by Justin Ide
Health
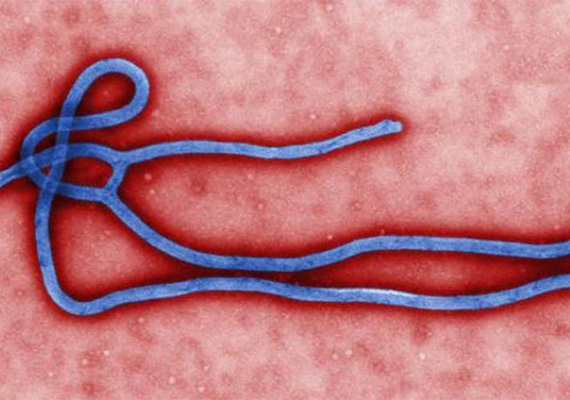
Understanding Ebola
Harvard’s VanRooyen explains how disease works and how to make headway against it
Though a few Ebola-infected Americans have begun returning home from the epidemic in West Africa, U.S. medical experts believe that there is still little risk that the epidemic will gain hold here. Key questions, however, include how much help U.S. organizations will give to overwhelmed medical facilities in affected nations, and how quickly personnel there can get the disease under control.
To better understand the disease and the threat it presents, the Gazette spoke with Michael VanRooyen, director of the Harvard Humanitarian Initiative (HHI), which works to improve humanitarian response to disasters around the world through training, research, and by developing tools that put information at responders’ fingertips.
VanRooyen, a professor at Harvard Medical School and the Harvard School of Public Health and vice chairman of Harvard-affiliated Brigham and Women’s Hospital’s Department of Emergency Medicine, has extensive experience responding to humanitarian crises, from the Rwandan genocide to the turmoil in the eastern Democratic Republic of the Congo to the 2010 Haiti earthquake, when HHI and physicians from Harvard-affiliated hospitals erected a field hospital to handle the injured. Here are his thoughts.
GAZETTE: What’s the most important thing for the American public to understand about this outbreak?
VANROOYEN: I think most important is that there’s no cause for panic. We have experts who understand the spread of this virus and how to protect the public from it. When the [nonprofit] Samaritan’s Purse, for example, evacuates somebody and has them sent to Atlanta for treatment and surveillance, it does not pose an epidemic risk in the United States. That’s probably first and most important.
Second, the countries that we work in, like Sierra Leone and Liberia and Guinea, depend on us to lead the response. This epidemic has rapidly exceeded the capacity of local hospitals and health institutions, and we should mobilize resources to help. We have well-trained experts and significant resources to provide a robust response by the CDC [Centers for Disease Control and Prevention], as well as NGOs [nongovernmental organizations], and even the private sector. We need to quickly mobilize people to help control the epidemic and undertake a public health campaign.
GAZETTE: What are the biggest medical needs?
VANROOYEN: We have close colleagues working in Liberia and Sierra Leone, and they have indicated two major areas of need.
First is greater technical support of the health care delivery program for better hospital treatment, case management, and quarantine. Some of the hospitals in Liberia are closing down or severely reducing their capacity because they don’t have gowns, gloves, respirators, or other protective gear. One critical essential need is the personal protective gear that will allow front-line health care workers to safely treat infected patients. Linked with that is medical expertise: It is essential to send physicians, nurses, and public-health experts who have significant expertise and some prior experience with acute onset epidemics. The right people and supplies can go a long way in stemming the spread of the disease.
The second area that we really need to enhance is community education. The virus spreads from person to person through intimate contact, such as feces and blood and preparing bodies for burial. This puts health care workers, close family members, and those preparing the dead for burial at risk. Although there has been an aggressive campaign in recent years, in some places, like Sierra Leone and Liberia, it’s [backfired and] actually caused people to be suspicious of health care workers.
GAZETTE: We’re hearing that the disease is hard to spread and not a big danger to the U.S., and yet it does seem to be spreading in Africa. Why it isn’t considered a danger here?
VANROOYEN: The disease spreads — and the CDC has confirmed this — through very close personal contact, blood and feces. As long as people are under proper care and appropriate precautions are taken, there’s no reason to think we can’t control the transmission of the virus. So in that sense, it’s not like SARS [severe acute respiratory syndrome] or MERS [Middle East respiratory syndrome], for example, where we would worry about an epidemic spreading in the United States.
GAZETTE: Because SARS is respiratory?
VANROOYEN: Exactly. With SARS or influenza, the disease can spread through casual contact, such as on a bus, train, or plane. But fortunately, Ebola is only spread by patients who have become symptomatic, and then only spread through close contact with blood, feces, and other bodily fluids. If you have no symptoms, you don’t spread the illness. If we are carefully screening patients who have been exposed to Ebola and become ill, the transmission can be controlled. I would agree with the CDC that the risk of an epidemic spreading in the United States is very low.
GAZETTE: What has your involvement been so far?
VANROOYEN: HHI is hosting a symposium of ambassadors of five African nations, including Sierra Leone and Liberia, to discuss some of the challenges and unmet needs regarding the epidemic, and ways to better prepare their health and public health systems. The meeting will bring together several experts in health systems and public health communications. The meeting will be the first of several, and we hope to get the participation of CDC and several organizations with experience in managing the epidemic.
I am also working closely with my colleagues from Samaritan’s Purse, who have been leading medical management efforts in Liberia. My colleague and long-time friend Ken Isaacs, the vice president of Samaritan’s Purse, has been deeply concerned with the lack of medical capacity in these West African countries and the complexities of managing those returning to the U.S.
Recently, we’ve been approached by several organizations, including the American Red Cross and the International Rescue Committee, to send health personnel — to Sierra Leone in particular — to run the health programs there for the Ebola epidemic. Harvard has suspended all nonessential travel to those areas and I haven’t sent anybody yet. That being said, we’re exploring it. They [would be working with] strong NGOs, with solid leadership, but we have not yet committed personnel to the area.
GAZETTE: So it would be a Harvard person associated with HHI working for one of these NGOs?
VANROOYEN: All clinical relief work we do is through our partner hospitals. Although these physicians are academically affiliated with HHI, they are performing clinical work as a hospital physician from the Brigham or other Harvard-affiliated hospital.
GAZETTE: Is there a particular specialty they’re looking for?
VANROOYEN: They’re primarily looking for emergency-medicine physicians with relief experience, although in this case infectious disease specialists and those with experience managing an epidemic would be most helpful. Although we have a group of emergency physicians that have had specialty training in humanitarian medicine, few have experience in managing an epidemic.
GAZETTE: They have experience overseas and in crisis situations?
VANROOYEN: Yes. Most have specific training in humanitarian assistance as well as significant experience with multiple deployments in refugee health settings in conflict and disasters. Obviously, the Ebola epidemic is unique and requires a specific training.
GAZETTE: What’s the role of an academic institution like Harvard and our affiliated hospitals, and what should it be in this sort of a situation?
VANROOYEN: In general, the role of an academic institution is not to provide clinical services on the ground in an epidemic, but to provide other types of support for NGOs, through research and information management. Although we may send hospital medical staff to work in medical facilities, the role of Harvard is to investigate and address the broader implications of the epidemic, such as the social and political implications of this epidemic in Sierra Leone, which already has an unstable government. There are significant collateral issues that can lead to political instability and public mistrust of the government.
We also provide better data collection tools for organizations to gather and share data real-time. Organizations responding to these crises may not place a priority on data collection, management, analysis, and sharing, and we have worked in both Sierra Leone and Liberia in mapping population needs and disease patterns. As with other humanitarian crises around the world, HHI and Harvard can play an important role in educating responders, understanding social, political, and human rights dimensions, and helping to optimize future responses.





